



Medial Tibial Stress Syndrome
What is Medial Tibial Stress Syndrome?
Medial tibial stress syndrome (MTSS), also known as “shin splints”, is an overuse injury that causes pain at the front of the shin with exercise. MTSS is an early stress injury along a spectrum that includes tibial stress fractures. It is most common in runners, jumping athletes, and military personnel-- individuals which undergo recurrent impact exercise.
Differential diagnosis of MTSS requires clinicians to distinguish MTSS from tibial stress fractures, exertional compartment syndrome, peripheral vascular disease or popliteal artery entrapment, and other less common causes of exertional pain in the lower extremities, including muscle or fascia involvement or nerve entrapment syndromes.
Medial Tibial Stress Syndrome (Shin Splints) Background
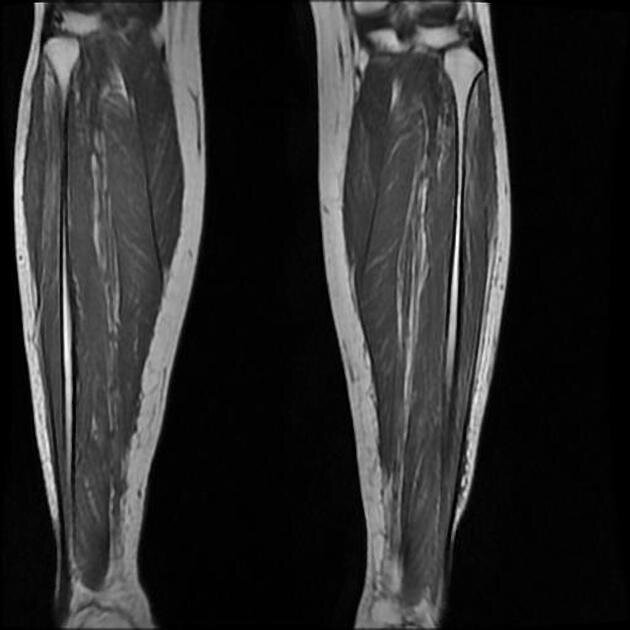
There are 4 muscle compartments in the lower leg, each containing several muscles and their attachment to the tibia (shin bone) and fibula (a long, thin bone on the outside of the lower leg). The underlying process that results in MTSS is related to the accumulation of microdamage at the attachment of these muscles to the bone. Tenderness and pain typically corresponds to inflammation at these attachment sites (periostitis), and may be associated with dysfunction of the corresponding muscles and subsequent damage to the bone. It remains unclear if periostitis occurs before the bony microtrauma or after.
“Shin Splints or Medial Tibial Stress Syndrome can be a very frustrating injury for even the most successful runners. I have seen this injury affect high level runners as they adjust mileage, have changes in sleep, diet, or mechanics alterations.”

What Causes Medial Tibial Stress Syndrome (Shin Splints)?
The cause of MTSS is often due to multiple factors, and frequently includes a combination of training errors, muscle dysfunction, and biomechanical factors.
Training errors: A rapid change in frequency or intensity of activity is the most common cause of overload-type injuries. This includes changes in mileage, pace, type of activity, and even terrain or footwear. Overuse injuries occur when the amount of load through the joint for a specific movement exceeds the tissue’s ability to recover on a timely basis.
Muscle dysfunction: Imbalance and inflexibility in several key muscles in the lower leg may make an individual more prone to muscle fatigue, leading to altered movement mechanics and increased strain on the tibia. Tibialis anterior and posterior are the most frequently involved muscles; their attachment sites correlate to the most common locations of pain.
Biomechanical factors: Abnormalities in foot and ankle mobility, tibial torsion, knee angle, and even leg-length discrepancy can alter movement mechanics and result in increased strain on the tibia as well. This is compounded by the presence of prior unresolved running injuries.
“The most common causes I see in clinic are running training errors, poor or old running shoes, and ramping up weekly mileage too fast. ”
Several additional factors may increase your risk of MTSS:
Women are more likely than men to develop MTSS due to the higher incidence of osteoporosis, in the spectrum of decreased bone density. This is especially common in female athletes who present with the “female athlete triad” (osteoporosis, disordered eating, and amenorrhea). Decreased bone density reduces the threshold at which stress fractures may occur, as the bony tissue does not hold up as well against repetitive stresses.
Individuals who are overweight are also more susceptible to MTSS, as are those who carry heavy loads on a regular basis (military personnel, firefighters). Increased forces through the bony structures, especially with repetitive impact activities, can result in overload injuries.
Dr. Jonathan Hall, MD at ProOrtho in Kirkland when asked stated, “New shoes can be a culprit due to a changes in forces. In addition harder surfaces (such as pavement) that increase the contact forces between the limb and the ground may also play a part. Your lower limbs, which include your feet, ankles, shins, knees, thighs and hips and all the ligaments and muscles that cross them, and as an extension both your shoes and your lower back, provide the shock absorption during high impact activities like jogging, running and sports. When any of those are not doing their part the rest of the system has to make up for it. And the tibia (your shin bone) seems to be one of the first (along with your plantar fascia of your heel) to pay the price.” Dr. Peter Vincent from Washington Foot and Ankle adds, “When I see young cross-country athletes starting season de-conditioned the are strong candidates for injury.”
“Physical therapy is an excellent way to do this. Start from the ground and work your way up. Running surface? Shoes? Foot alignment or overall limb alignment problems? And then get help to evaluate the mechanics of your gait.”
Dr. Troy Henning, DO from Swedish Hospital supported similar thoughts. He states that, “MTSS in the lower leg in runners can be related to poor neuromuscular control of the hip girdle and ankle stabilizers/foot intrinsics-- essentially excessive hip adduction, as seen with weak hip abductor/adductor balance”. What does this mean? Runners will need to achieve more balance between strength and flexibility on the inner and outer hip. Dr. Henning adds, “[Weakness in] core muscles can allow the pelvis to drop excessively on the swing side, and lead to hip adduction on the stance leg. What about the foot and ankle, you might ask? Dr. Henning states that, “If the foot is going into excessive pronation because of relatively weak tibialis posterior/foot intrinsics or tight triceps surae, the tibia may internally rotate more than what is ideal.” This would lead to a tensioning and consistently eccentrically loading the muscles of the lower leg.

Other factors that can increase your risk of MTSSS include:
Training errors: A sudden change in frequency or intensity of activity can result in an overuse injury. In the case of MTSS, repetitive movements through doorsflexion and plantar flexion put stress on the involved structures. Although these movements are a component of normal daily life, overuse injuries occur when the amount of load through the joint exceeds the tissue’s ability to recover on a timely basis.
Anatomical factors: The geometry of your body affects the distribution of load through specific structures. Individuals with differences in limb length, an abnormal knee angle (either “knock kneed” or “bow legged”), excessive foot pronation (inward collapse of the midfoot), weak hip musculature, or poor mechanics.
Biomechanical factors: Structural differences aside, the way your body moves may also affect the distribution of load through the tibia and nearby tissues. This includes muscle weakness or relative imbalance among the quadriceps, hamstrings, or gluteus muscles. Additionally, poor motor control may result in increased landing forces in each step or cycle of sport-specific movements. Any one of these may contribute to the development of MTSS.
We asked longtime colleague and prominent physiatrist at Swedish, Dr. Irene Young her thoughts what she sees in her practice. Dr. Young is a runner herself as well as her husband. She states, “Common causes of MTSS in our patients include muscle imbalances, anatomical variation and training changes.”
“MTSS can be frustrating to treat for some athletes as it can take a considerable amount of time and rehabilitation to treat the condition. Mainstay treatments often involve relative rest, NSAIDs, physical therapy, shoe replacement, orthotics, and gait retraining.”
Common Medial Tibial Stress Syndrome Symptoms

MTSS most commonly presents with tenderness, soreness, or dull pain along the lower leg, and is sometimes associated with mild swelling. This may occur at the front of the leg or even toward the inner/back of the leg. This pain is often worse at the beginning of the exercise, and may initially go away when you rest. As the injury progresses, the pain will occur with less intense activities and may occur even at rest.
When asked about the typical clinical presentation that he sees in office Dr. Vincent states, commonly I see an over pronated foot and/or a rigid foot (ie cavus ). Many times with runners there is over controlled or under controlled foot mechanics.”
“An athlete with great biomechanics can develop poor biomechanics when fatigued—get sloppy. One of the most common injuries in sport. MTSS should be self-limiting by decreasing/stopping activity, icing, stretching, physical therapy and REST—if one follows those guidelines and still has pain walking or early in a run after 3-6 weeks they should consider seeing a physician to rule out a stress fracture or compartment syndrome”

How Can Physical Therapy Help Medial Tibial Stress Syndrome (MTSS) / Shin Splints?
Physical therapy can evaluate the cause of your pain and get you back on your feet and on the road to recovery. Due to the many root causes of MTSS, treatment is unique to the individual. Treatments may include:
Modification of training programs including intensity, frequency, and duration and education about low-impact and cross-training exercises during your recovery
Strength training focusing on hip stabilizing groups to decrease stress in the lower leg, and exercises that increase arch and shin muscle strength to address overpronation at the foot during contact / strike and stance phase (single leg support)
Sport-specific gait and movement retraining to improve the dynamic alignment of your hips, knees, and ankle, so that you can better perform activities including walking, running, and jumping
Stretching and soft tissue mobilization to increase flexibility of your calf and foot muscles
Manual therapy and taping to directly address specific biomechanics
Footwear and orthoses to support improved alignment of your lower extremities during daily activities and sport-related movement
Ice, active recovery, and appropriate rest to reduce pain and inflammation
If these areas are ineffective then both Dr. Robert, Dr. Hall, and Dr. Vincent would recommend a treatment of Shock Wave therapy to the effected region.
We were fortunate to have lifelong runner Dr. Ghislaine Robert, MD weigh in. Dr. Robert is a redmond physician and former Canadian Track and Field physician. She sees a significant amount of local runners each year complaining of “shin pain”. Dr. Robert adds that physical therapy can help in addressing soft tissue restrictions, joint mobilities, shoe selection, possibly orthotics if indicated, gradual coaching on the return to running, and help in selecting a running coach. If needed a physician like Robert can help rule out a stress reaction or possible stress fracture through diagnostic testing.
AUTHOR:
CONTRIBUTORS:
Dr. Bob Adams, DO, Ret. Head Medical Physician USA Track & Field
Dr. Jonathan Hall, MD
Dr. Troy Henning, DO
Dr. Larry Maurer, DPM
Dr. Ghislaine Robert, MD, Frm Canadian Track & Field Team Physician
Dr. Peter Vincent, DPM
Dr. Irene Young, MD
Ben Wobker, PT, MSPT, CSCS, CFSC, SFMA
More Related Articles
References
Shin Splints. Mayo Clinic. 2020. Web. https://www.mayoclinic.org/diseases-conditions/shin-splints/symptoms-causes/syc-20354105
McClure CJ, Oh R. Medial Tibial Stress Syndrome. StatPearls. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538479/
Galbraith, RM and Lavallee, ME. Medial Tibial Stress Syndrome: Conservative Treatment Options. Curr Rev Musculoskelet Med. 2009 Sep; 2(3): 127–133. doi: 10.1007/s12178-009-9055-6.
Winkelmann, ZK; Anderson, D; Games, KE; and Eberman, LE. Risk Factors for Medial Tibial Stress Syndrome in Active Individuals: An Evidence-Based Review. Journal of Athletic Training. 2016; 51(12):1049-1052. doi: 10.4085/1062-6050-51.12.13.
Barton cj, Bonanno dr, Carr j, Neal bs, Malliaras p, Franklyn-miller a, Menz hb. Running Retraining to treat lower limb injuries: a mixed-methods study of current evidence synthesised with expert opinion. br j sports med. 2016 feb 16. pii: bjsports-2015-095278. doi: 10.1136/bjsports-2015-095278. [epub ahead of print] review. pmid:26884223
Luedke le, Heiderscheit bc, Williams ds, Rauh mj. Influence of step rate on shin injury and anterior knee pain in high school runners. med sci sports exerc. 2016 jan 26. [epub ahead of print] pmid: 2681815
Willy rw, Buchenic l, Rogacki k, Ackerman j, Schmidt a, Willson jd. In-field gait retraining and mobile monitoring to address running biomechanics associated with tibial stress fracture. scand j med sci sports. 2016 feb;26(2):197-205. doi: 10.1111/sms.12413. epub 2015 feb 4. pmid: 25652871
Breen dt, Foster j, Falvey e, Franklyn-miller a. Gait re-training to alleviate the symptoms of anterior exertional lower leg pain: a case series. int j sports phys ther. 2015 feb;10(1):85-94. pmid:25709867